Osteoarthritis of the Acromioclavicular Joint | eorthopod.com
A Patient's Guide to Osteoarthritis of the Acromioclavicular Joint
Introduction
Some joints in the body are more likely to develop problems from normal wear and tear. Degeneration causes the cartilage that cushions the joint to wear out. This type of
arthritis is called
osteoarthritis. Doctors sometimes refer to this type of arthritis as
arthrosis.
The
acromioclavicular (AC) joint in the
shoulder is a common spot for osteoarthritis to develop in middle age. Degeneration of the
AC joint can be painful and can cause difficulty using the shoulder for everyday activities.
This guide will help you understand
- what the AC joint is and how it works
- the causes of pain and problems in the AC joint
- the treatments used for this condition
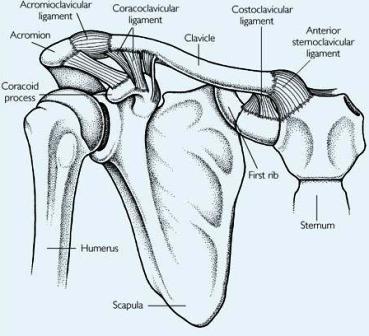
Anatomy

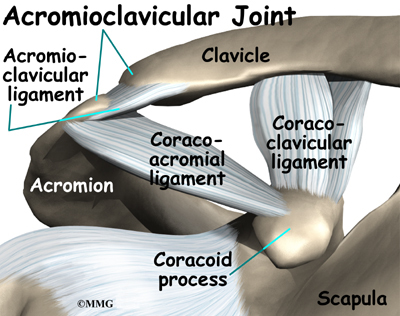
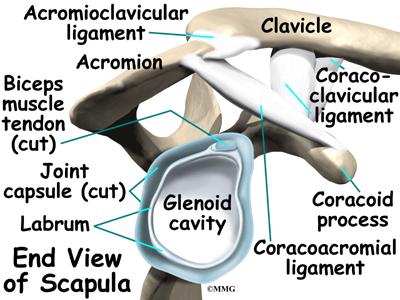
What exactly is the AC joint?
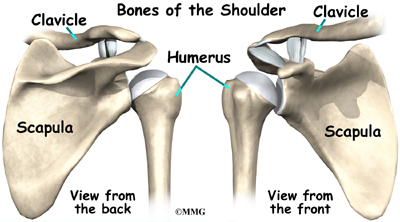
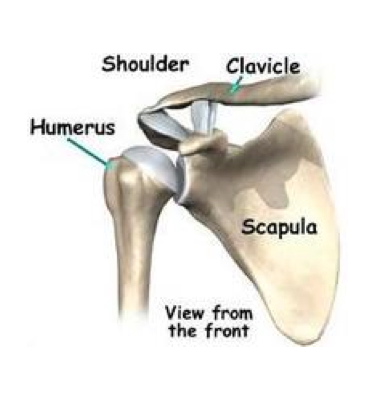
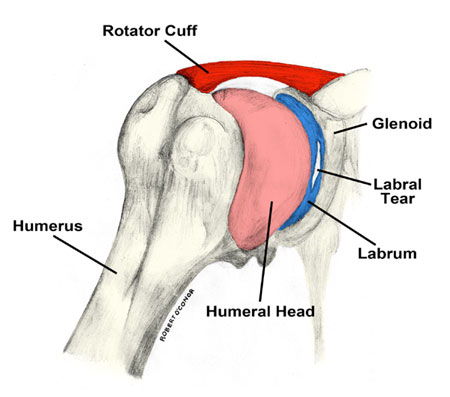
The shoulder is made up of three bones: the
scapula (shoulder blade), the
humerus (upper arm bone), and the
clavicle (collarbone).
The part of the scapula that makes up the roof of the shoulder and connects with the clavicle is called the
acromion.

The joint where the acromion and the clavicle join is the
AC joint.
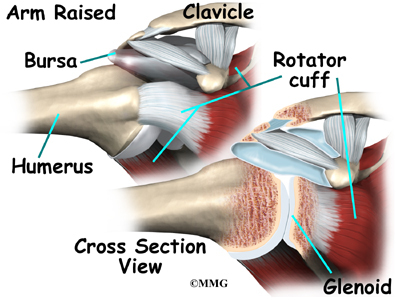
In some ways, the AC joint is like any other joint. It has two bones that need to connect but be flexible as well. The ends of the bones are covered with
articular cartilage. Articular cartilage provides a slick, rubbery surface that allows the bones to glide over each other as you move. Cartilage also functions as sort of a shock absorber.
However, the AC joint is different from joints like the
knee or ankle, because it doesn't need to move very much. The AC joint only needs to be flexible enough for the shoulder to move freely. The AC joint just shifts a bit as the shoulder moves.
View animation of shoulder movement
Related Document:
A Patient's Guide to Shoulder Anatomy
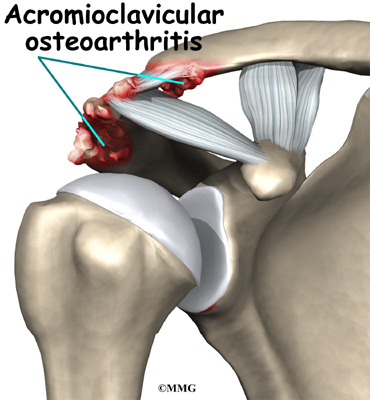
Causes
Why does degeneration of the AC joint occur?
We use our shoulder constantly. The resulting strain makes AC joint osteoarthritis a common disorder. The AC joint is under constant stress as the arm is used overhead. Weightlifters and others who repeatedly lift heavy amounts of weight overhead tend to have an increased incidence of the condition, and often at a younger age.
AC joint osteoarthritis may also develop following an injury to the joint, such as an AC joint separation. This injury is fairly common. A separation usually results from falling on the shoulder. The shoulder does heal, but many years later degeneration causes the AC joint to become painful.
Related Document:
A Patient's Guide to Acromioclavicular Joint Separation
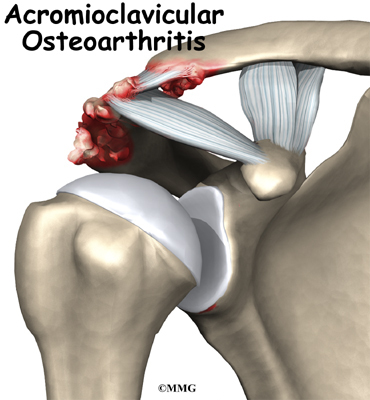
Symptoms
What are the symptoms of this condition?

In its early stages, AC joint osteoarthritis usually causes pain and tenderness in the front of the shoulder around the joint. The pain is often worse when the arm is brought across the chest, since this motion compresses the joint. The pain is vague and may spread to include the shoulder, the front of the chest, and the neck. If the joint has been injured in the past, there may be a bigger bump over the joint on the affected shoulder than on the unaffected shoulder. The joint may also click or snap as it moves.
Diagnosis
What tests will my doctor do?
Your doctor will want to get a detailed medical history, including questions about your condition and how it is affecting you. You will need to answer questions about past injuries to your shoulder. You may be asked to rate your pain on a scale of one to ten. Your doctor will also want to know how much your pain affects your daily tasks.
Diagnosis of AC joint osteoarthritis is usually made by physical examination. The AC joint is usually tender. A key finding is pain as the joint is compressed. To test for this, your arm is pulled gently across your chest. Your doctor may inject a local anesthetic such as
lidocaine into the joint. If the AC joint is the problem, the injection will temporarily reduce the pain.

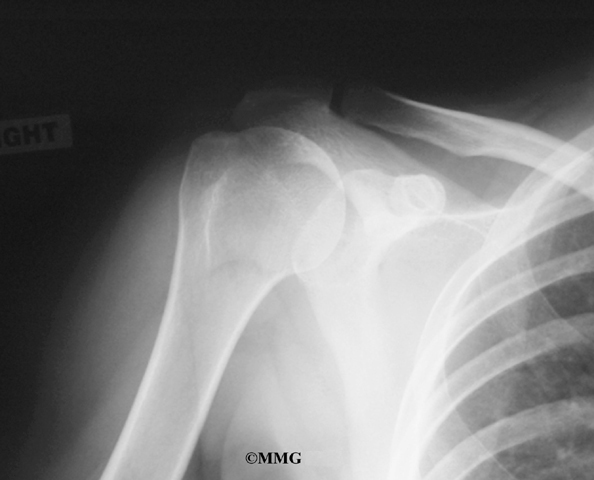
Your doctor may want to take X-rays of the AC joint. X-rays can show narrowing of the joint and bone spurs around the joint, which are signs of degeneration.
Treatment
What treatment options are available?
Nonsurgical Treatment
Initial treatment for AC joint osteoarthritis usually consists of rest and anti-inflammatory medications such as aspirin or ibuprofen. A rehabilitation program may be directed by a physical or occupational therapist. If the pain doesn't go away, an injection of
cortisone into the joint may help. Cortisone is a strong medication that decreases inflammation and reduces pain. Cortisone's effects are often temporary, but it can give very effective relief in the short term.
Related Document:
A Patient's Guide to Joint Injections for Arthritis
Surgery
If nonsurgical measures fail to relieve your pain, your doctor may recommend surgery.

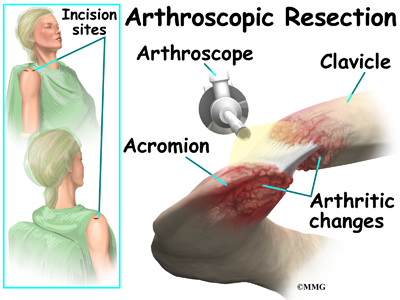
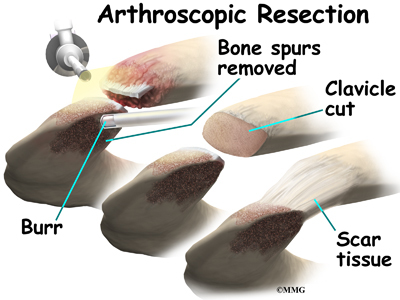
The most common procedure for AC joint osteoarthritis is
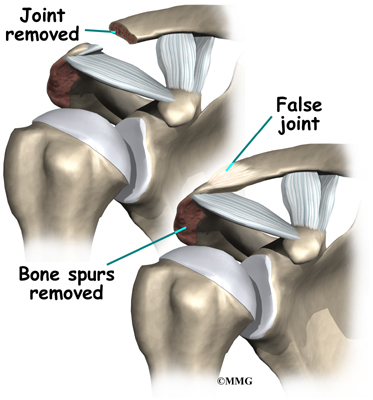
resection arthroplasty. A resection arthroplasty involves removing a small portion of the end of the clavicle. This leaves a space between the
acromion (the piece of the scapula that meets your shoulder) and the cut end of the clavicle, where the joint used to be. Your surgeon will take care not to remove too much of the end of the clavicle to prevent any damage to the ligaments holding the joint together.

Usually only a small portion is removed, less than one cm (about three-eighths of an inch). As your body heals, the joint is replaced by scar tissue. Remember, the AC joint doesn't move much, but it does need to be flexible. The scar tissue allows movement but stops the bone ends from rubbing together.
This procedure can be done in two ways. Today, it is more common to do this procedure using the arthroscope. An arthroscope is a slender tool with a tiny TV camera on the end. It lets the surgeon work in the joint through a very small incision. This may result in less damage to the normal tissues surrounding the joint, leading to faster healing and recovery.

The older
open method of performing this operation is done by making a small incision, less than two inches long, over the AC joint. The AC joint is very close to the surface of the skin and can be easily reached through a small incision. The surgeon can then use a special saw or other instrument to shave off a small portion of the end of the clavicle.
Rehabilitation
What should I expect after treatment?
Nonsurgical Rehabilitation
If you don't need surgery, range-of-motion exercises should be started as pain eases, followed by a program of strengthening. At first, exercises are done with the arm kept below shoulder level. The program advances to include strength exercises for the rotator cuff and shoulder blade muscles. The goal is to get your shoulder moving smoothly and to learn how to control your symptoms. You will probably progress to a home program within four to six weeks.
After Surgery
Your surgeon may have you wear a sling to support and protect the shoulder for a few days. A physical or occupational therapist will probably direct your recovery program. The first few therapy treatments will focus on controlling the pain and swelling from surgery. Ice and
electrical stimulation treatments may help. Your therapist may also use massage and other types of hands-on treatments to ease muscle spasm and pain.
Therapy can progress safely and quickly after a simple arthroscopic resection. Treatments start out with range-of-motion exercises and gradually work into active stretching and strengthening. You need to avoid doing too much, too quickly.
Therapy goes slower after surgeries where an incision is made through the shoulder muscles. Therapists usually wait up to two weeks before starting range-of-motion exercises. You will begin with passive exercises. In passive exercises, the
shoulder joint is moved, but your muscles stay relaxed. Your therapist gently moves your joint and gradually stretches your arm. You may be taught how to do passive exercises at home.
Active therapy starts after four to six weeks. Active range-of-motion exercises help you regain shoulder movement using your own muscle power. You might begin with light isometric strengthening exercises. These exercises work the muscles without straining the healing joint.
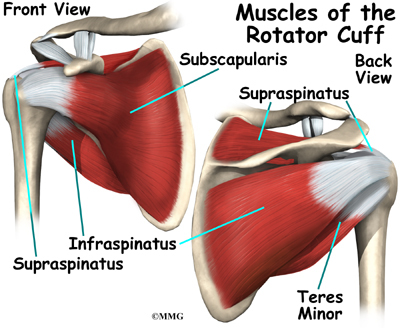
At about six weeks, you will start more active strengthening. Exercises will focus on improving strength and control of the rotator cuff muscles and the muscles around the shoulder blade. Your therapist will help you retrain these muscles to keep the ball of the humerus centered in the socket. This helps your shoulder move smoothly during all your activities.
Some of the exercises you'll do are designed to get your shoulder working in ways that are similar to your work tasks and sport activities. Your therapist will help you find ways to do your tasks that don't put too much stress on your shoulder. Before your therapy sessions end, your therapist will teach you a number of ways to avoid future problems.